
Sleep Paralysis as Threshold State: Between Dream and Waking, Self and Other
You wake. You cannot move. The body, still in REM atonia, has not received the signal of waking. The mind is conscious. The body is paralysed. The gap between them is the threshold–neither sleep nor waking, neither dream nor reality, neither self nor other. This is sleep paralysis. The culture calls it nightmare. The tradition calls it opportunity.
The body follows its own protocols with neurological precision. The consciousness, that restless observer, has arrived early, finding the motor systems still locked in their nightly routine. Meanwhile, the physical form remains bound by the protocols of the nervous system, rigid as a sealed vessel. The threshold is not merely a gap but a territory–a liminal space where the usual boundaries of being are suspended, and other modes of perception may claim temporary attention.
Table of Contents
- The Phenomenology Is Specific
- The Neuroscience of the Threshold
- The Tradition Recognises the Threshold
- The Old Hag Syndrome: Cultural Archives
- The Navigation Requires Preparation
- Sleep Paralysis as Gateway
- The Dangers Are Real
- The Thread Extended
- Frequently Asked Questions
- Further Reading
- References and Sources
The Phenomenology Is Specific
The sequence is predictable. The waking. The realisation of immobility. The attempt to move, failed. The panic, rising. Then–the shift. The attention, denied external action, turns inward. And something is there.
The presence is not imagined. It is perceived. The figure, often shadowed, often feminine, often ancient, occupies the space at the threshold. The culture names it: the old hag, the incubus, the succubus, the jinn, the alien. The name is post-hoc. The experience precedes naming, yet the naming attempts to capture something essential about the nature of the encounter. The figure often appears not as a random intruder but as something with purpose–a presence that observes, evaluates, or presses close. Reports consistently describe a sense of being scrutinised, as though one’s entire condition were under review by an intelligence that predates the self.
The interaction varies. Sometimes observation. Sometimes approach. Sometimes pressure, weight, the sense of intrusion. The terror is not optional. The body, vulnerable, responds with maximal alarm. The alarm, resisted, amplifies. The alarm, accepted, transforms. The key variable is not the presence but the response–whether the practitioner meets the threshold with recognition or with struggle.
The Neuroscience of the Threshold
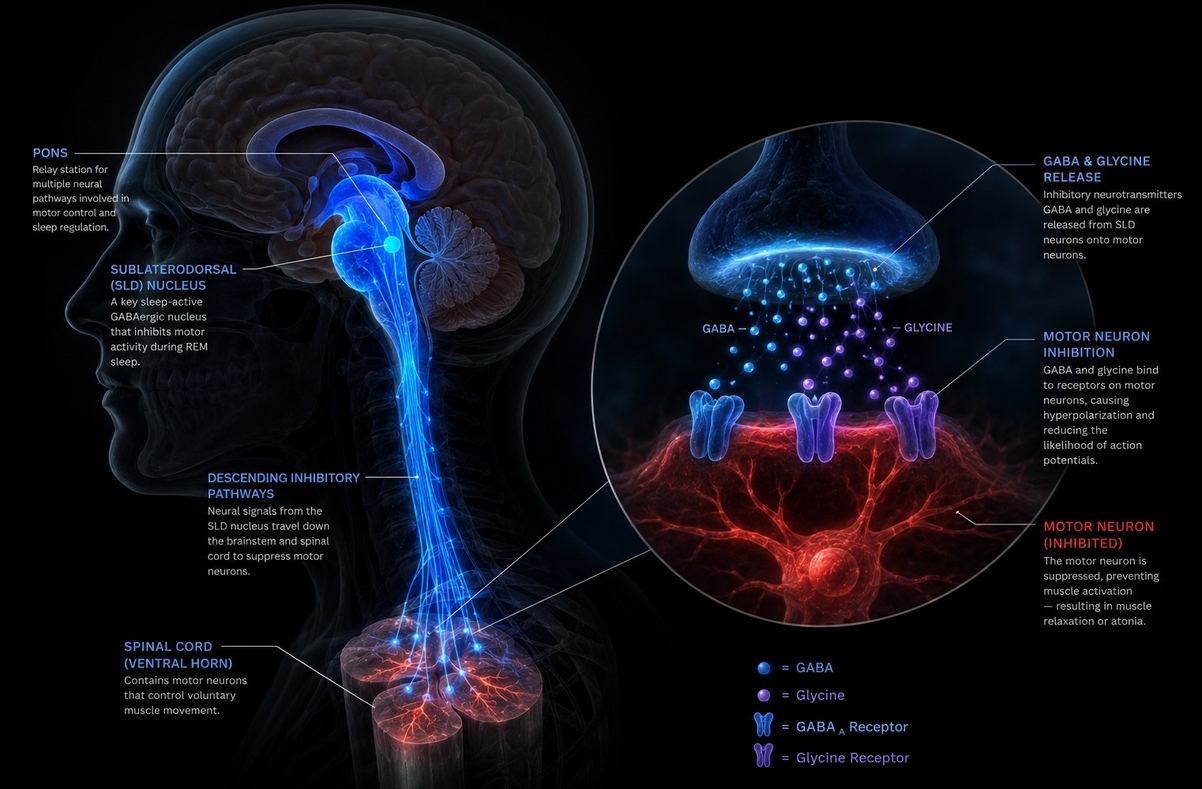
Modern neuroscience has mapped the mechanism with increasing precision. REM atonia–the paralysis that prevents us from acting out our dreams–is generated by the sublaterodorsal nucleus (SLD) in the pons. During ordinary REM sleep, the SLD releases GABA and glycine onto spinal motoneurons, inhibiting voluntary muscle activation. When we wake, the SLD normally disengages, and motor function returns. In sleep paralysis, cortical arousal occurs before the SLD releases its hold. The brain is awake; the body is not.
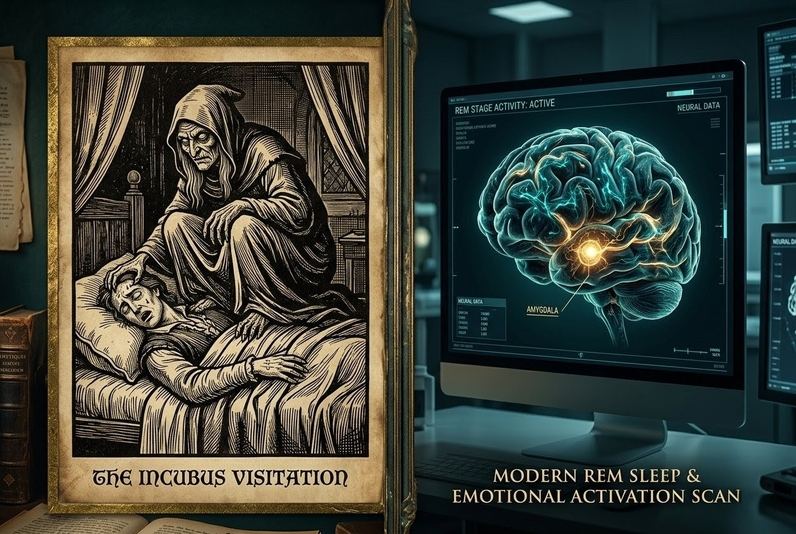
The terror has its own neurology. The amygdala, that ancient threat-detector, activates in response to the body’s vulnerability, flooding the system with adrenaline while the muscles remain chemically restrained. The central nucleus of the amygdala (CeA) exerts direct influence on REM regulation, and its hyperactivation during SP correlates strongly with the intensity of intruder hallucinations. The prefrontal cortex, responsible for rational assessment, is partially offline during the transition, leaving the amygdala’s alarm largely unmodulated.
Recent electrophysiological research has revealed something even more intriguing. Herrero and colleagues demonstrated that sleep paralysis shows increased beta and low-gamma activity compared to ordinary REM sleep, alongside reduced theta power. This pattern–termed “lucid paralysis”–suggests that SP is not merely a glitch but a distinct brain state, one that shares features with both waking consciousness and lucid dreaming. The brain, in other words, is not malfunctioning. It is occupying a genuine liminal state–one that may have been cultivated deliberately in traditions that recognised its potential.
The Tradition Recognises the Threshold
The shamanic initiation often includes paralysis. The candidate, immobilised, encounters the spirits. The encounter, survived, establishes relationship. The relationship, cultivated, becomes practice. The paralysis is not pathology. It is threshold–the necessary passage between ordinary and non-ordinary consciousness.
The Tibetan tradition describes milam–dream yoga. The practitioner learns to recognise the dream state, to maintain consciousness through transition, to encounter the deities without terror. The sleep paralysis, uninvited, offers the same opportunity. The recognition, applied, transforms the encounter. In the Tibetan system, the throat chakra is associated with dreams; the subtle energy channels converge there during sleep. The paralysis, experienced at the threshold between waking and dreaming, may represent a spontaneous activation of these channels–an unbidden opening of the same doorway the yogi cultivates through years of practice.
The Western esoteric tradition describes the astral body, the subtle vehicle, the double. The paralysis is separation–partial, involuntary, uncontrolled. The figure perceived is projection, or visitation, or the self seen from outside. The interpretation varies. The experience is constant. The Hermetic axiom “as above, so below” suggests that the interior and exterior worlds mirror each other; in the threshold state, the mirror becomes visible.
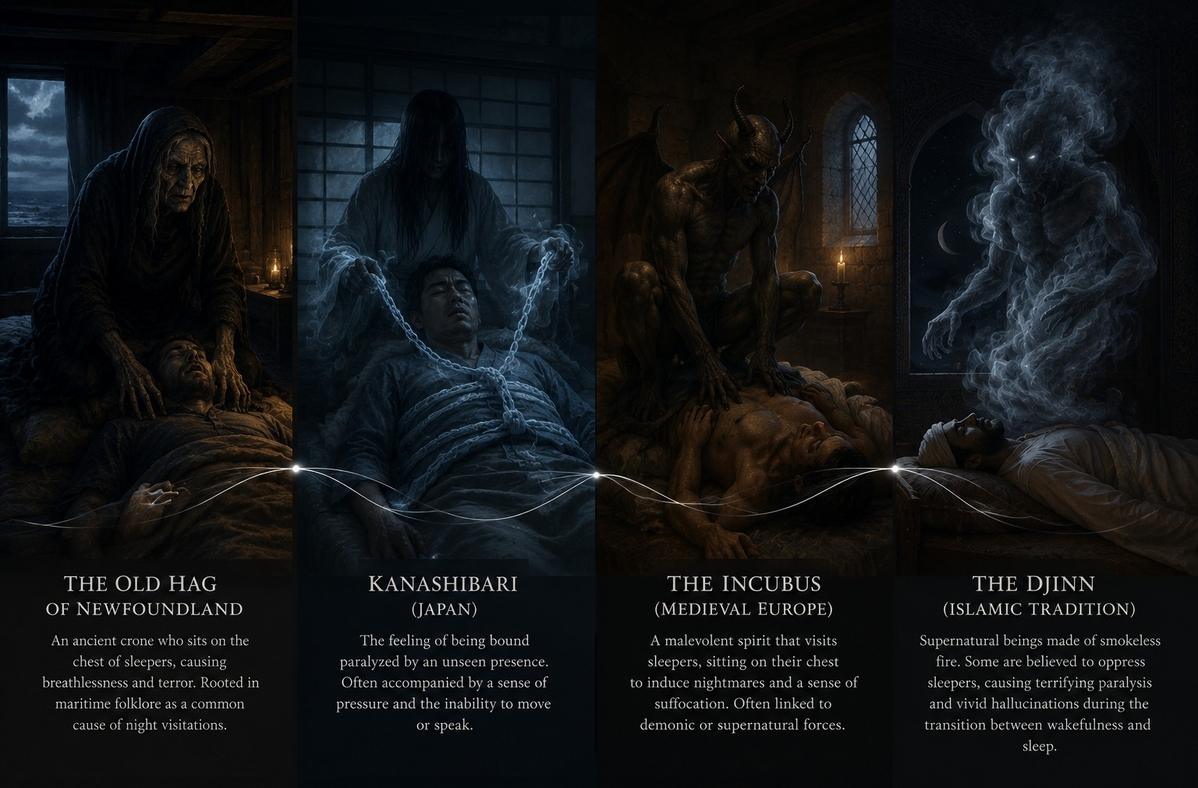
The Japanese tradition names it kanashibari–“bound in metal”–attributing the immobility to spiritual interference. The Haitian Vodou tradition knows it as the cauchemar, the crushing spirit that rides the sleeper. Medieval Europe catalogued it as the incubus or succubus–entities that not only observed but pressed upon the chest, extracting something vital. Newfoundland’s oral archives preserve the “Old Hag,” a figure who sits upon the sleeper and steals breath. In South Asia, the bhut or djinn is blamed; in Egypt, the al-qarin; in Nigeria, the ogun oru (“nocturnal warfare”). Each culture maintains different symbolic systems for the same encounter, different masks for the same threshold guardian.
The Old Hag Syndrome: Cultural Archives of the Threshold
The consistency of these reports across unconnected civilisations suggests not a shared folklore but a shared facility–a common room in the architecture of consciousness where the same presence appears regardless of the visitor’s origin. The “Old Hag” is not merely a nightmare figure; she is the anthropomorphised recognition of the threshold itself.
In the Gnostic framework, this figure might represent the archonic guardian–the border agent who examines credentials before allowing passage beyond the material realm. The pressure on the chest, the difficulty breathing, the sense of imminent doom–these are not symptoms to be medicated but signals to be interpreted. The hag sits not as tormentor but as gatekeeper, and the key she demands is recognition: the acknowledgment that one stands at a border, that ordinary consciousness has limits, and that beyond those limits lie territories requiring different credentials.
Yet the gatekeeper is not necessarily hostile. In many traditional accounts, the entity becomes benevolent once the sleeper ceases to struggle. The Japanese kanashibari can be dispelled by reciting a sutra or calling the entity’s name. The Newfoundland Hag retreats when the sleeper manages to move a single finger. The medieval incubus, resisted with prayer, dissolves. The pattern is consistent: resistance amplifies the terror; acceptance transforms the encounter. The threshold, approached with recognition, becomes a doorway rather than a wall.
The Navigation Requires Preparation
The paralysis, uninvited, cannot be chosen. But the response can be prepared. The preparation is not technique. It is orientation–the cultivation of relationship to the liminal, the acceptance of vulnerability, the recognition that the threshold is not enemy.
First, the Acceptance of Immobility
The struggle against paralysis amplifies terror. The acceptance, paradoxically, enables release. The body, unresisted, completes its transition. The paralysis, endured, becomes passage. The physiological mechanism is straightforward: struggle increases sympathetic arousal, which intensifies the amygdala’s threat response. Calm, conversely, allows the pons to complete its release sequence. The body is not broken; it is simply running on a different schedule.
Second, the Direction of Attention
The figure perceived, however terrifying, is not necessarily hostile. Reports consistently describe the entity standing to the left, hovering above, or pressing upon the chest. These are not random positions but orientations within the subtle architecture of the threshold. The attention, directed with curiosity rather than fear, transforms the encounter. The presence, met with recognition, may recognise in return. The question is not “what is attacking me?” but “what is being revealed?”
Third, the Cultivation of Breath
The breath, in paralysis, is the one voluntary function remaining. The breath, slowed, signals safety to the amygdala. The terror, reduced, enables clarity. The clarity, sustained, enables encounter. The diaphragm remains under partial voluntary control even when limb muscles are locked. Slow, deliberate breathing–particularly extending the exhalation–activates the parasympathetic nervous system, counteracting the adrenaline surge that makes the experience unbearable.
Fourth, the Return Without Haste
The waking, forced, produces dissociation. The waking, allowed, produces integration. The experience, carried into ordinary consciousness, becomes resource rather than trauma. The practitioner who rises abruptly, heart pounding, encodes the episode as threat. The practitioner who allows the transition to complete, who lies still for a few moments after movement returns, encodes it as passage.

Sleep Paralysis as Gateway
For those who learn to navigate the threshold, sleep paralysis becomes not a disorder but a doorway. The same electrophysiological signature–reduced theta, increased beta/gamma, cortical arousal with motor inhibition–is the signature of the lucid dream and the out-of-body experience. The practitioner who remains calm during SP can often transition directly into a lucid dream by visualising a scene and allowing the dream body to form. Alternatively, the sensation of floating or rising–common during SP–can be cultivated into a deliberate out-of-body experience.
The Tibetan tradition formalises this in the practice of milam, where the yogi learns to recognise the “clear light” at the moment of falling asleep and to maintain awareness through the dissolution of ordinary perception. Sleep paralysis, for the unprepared, is a terrifying intrusion. For the prepared, it is an involuntary glimpse of the same territory the yogi cultivates voluntarily. The difference is not the state but the relationship to it.
Research on out-of-body experiences (OBEs) confirms that many spontaneous OBEs begin from sleep paralysis. The sensation of the “phantom body” floating above the physical form, the silver cord connecting the two, the perception of the room from an elevated perspective–all are phenomenologically consistent with the SP-to-OBE transition. Whether this represents a genuine separation of subtle from physical body, or a constructed perceptual experience generated by the temporoparietal junction, remains an open question. What is certain is that the experience is real to the experiencer, and that its transformative potential is independent of its ontological status.

The Dangers Are Real
The paralysis is not harmless. The terror, unmanageable, produces trauma. The presence, interpreted as demonic, produces religious crisis. The experience, repeated without integration, produces sleep disorder, anxiety, depression. The practitioner who romanticises the threshold without respecting its intensity risks psychological harm.
The medicalisation is also danger. The sleep paralysis, diagnosed, becomes pathology. The medication, prescribed, suppresses the threshold. The opportunity, lost, produces the safety of ordinary consciousness–and the poverty of that safety. To render the threshold invisible through pharmaceutical management is to accept a flattened existence, to renounce the vertical dimension entirely. Yet the opposite error–refusing all medical intervention while suffering repeated, unintegrated episodes–is equally destructive.
The middle path is discrimination. The physiology acknowledged. The meaning explored. The experience integrated. The threshold, navigated, becomes gateway. The gateway, repeated, becomes practice. The practice, sustained, produces the capacity to remain conscious through transitions that ordinarily obliterate awareness.
The Thread Extended

The sleep paralysis is not the thread. It is condition–the temporary failure of the usual separation between states, the brief visibility of the architecture beneath ordinary consciousness. The thread is recognition. The recognition that the threshold is real, that the encounter is possible, that the ordinary is not absolute.
The practitioner, prepared, uses the paralysis. The practitioner, unprepared, is used by it. The difference is not control. It is direction–the continued orientation toward the thread, even in involuntary experience, even in terror, even in the dark. The paralysis is not the destination; it is the customs checkpoint. One does not linger there, but one must pass through with gaze steady, with the recognition that the presence who examines you is, ultimately, another face of the self’s own deepest authority.

You wake. You cannot move. The threshold opens. The thread continues regardless.
Read With Discernment
This article touches material where experience, interpretation and symbolic language can easily blur. Read slowly, compare sources, and keep your own discernment intact.
- Editorial Principles — how ZenithEye separates source, interpretation and lived experience.
- Start Here — the reader guide for the wider archive.
- States of Knowing — altered states, dreams, consciousness, perception and direct experience.
- The Transformation — integration, grounding, spiritual emergence and return to ordinary life.
Frequently Asked Questions
What exactly is sleep paralysis and why does it occur?
Sleep paralysis occurs when REM atonia–the body’s natural paralysis during dream sleep–persists into waking consciousness. Physiologically, the brain has awakened while the body remains in its protective immobile state, governed by the sublaterodorsal (SLD) nucleus in the pons. This creates a threshold condition: you are conscious but cannot move, caught between sleep and waking.
Is the entity experienced during sleep paralysis real or just a hallucination?
The question assumes a distinction that the threshold state does not recognise. The presence is perceived, not imagined–it occupies the same perceptual bandwidth as ordinary reality. Neuroscience attributes the intruder hallucination to amygdala hyperactivation in response to vulnerability. Whether this represents an external autonomous entity, a projection of consciousness, or the self seen from outside remains the mystery of the threshold.
Can sleep paralysis be transformed into a spiritual practice?
Yes. Tibetan dream yoga (milam) and various shamanic traditions recognise sleep paralysis as an involuntary entry into the threshold state. By shifting from resistance to recognition–accepting the immobility, directing attention with curiosity rather than terror, and cultivating slow breath–the practitioner can transform the encounter from trauma to passage. Many experienced practitioners use SP as a launchpad for lucid dreaming or out-of-body experience.
Why does sleep paralysis cause a feeling of pressure on the chest?
This sensation results from the combination of restricted breathing during REM sleep and the amygdala’s threat response activating while the chest muscles remain paralysed. The brain interprets the inability to breathe deeply as external pressure. Cultures name this weight differently–the incubus, the Old Hag, kanashibari–but the physiological mechanism is universal.
How can I prevent sleep paralysis from happening?
While irregular sleep patterns, stress, and supine sleeping positions correlate with episodes, prevention is not always desirable for those working with threshold states. The medical approach suppresses the experience; the contemplative approach prepares for it. If cessation is necessary, regular sleep schedules, side-sleeping, stress reduction, and avoiding alcohol before bed may reduce frequency.
Is sleep paralysis related to lucid dreaming?
They share the same border territory. Both represent dissociations between consciousness and the physical body. Sleep paralysis is an involuntary threshold crossing; lucid dreaming is a cultivated one. Electrophysiologically, SP shows increased beta and low-gamma activity similar to lucid dreaming states. Many practitioners deliberately use the paralysis state as a launchpad for conscious astral projection or dream yoga.
Are there dangers to experiencing sleep paralysis regularly?
Unintegrated experiences can produce trauma, sleep disorders, anxiety, or religious crisis. However, the greater danger may be medicalisation–suppressing these threshold encounters with medication eliminates the opportunity for integration. The middle path requires discrimination: acknowledging the physiology while exploring the meaning. If episodes produce persistent distress or functional impairment, consult a sleep specialist.
Further Reading
- States of Knowing: What Happens When Consciousness No Longer Belongs to You — The full phenomenological map of non-ordinary states and their clinical correlates.
- Hypnagogia: The Threshold State Between Waking and Sleep — The creative potential of the liminal mind at the border of consciousness.
- Lucid Dreaming as Practice Platform: Conscious Within the Dream — How Tibetan dream yoga cultivates the same territory that sleep paralysis reveals involuntarily.
- The Physiology of Mystical Experience: What Actually Changes in the Brain — The neurobiology distinguishing spiritual states from pathology.
- The Transformation: What Actually Changes After Mystical Experience — From threshold encounter to grounded integration.
- Psychosis and Mysticism: The Shared Territory — Where diagnostic discernment meets spiritual breakthrough at the extreme edges.
- Default Mode Network Dissolution and the Self — Examines the neuroscience of ego dissolution and its parallels to threshold states.
- Spiritual Emergency: When Transformation Becomes Crisis — When threshold experiences accelerate beyond the capacity for integration.
- Integration Practices After Peak Experience — Practical grounding techniques for stabilising threshold encounters.
- Embodiment Practices: Grounding the Awakening — Why non-ordinary states require somatic anchoring to become transformative rather than destabilising.
References and Sources
The following sources represent the primary neuroscientific, clinical, and cross-cultural materials consulted in the preparation of this article.
Neuroscience and Sleep Research
- Herrero, J. L., et al. (2026). “Electrophysiological correlates of sleep paralysis reveal a distinct brain state.” Journal of Neuroscience.
- Brooks, P. L., & Peever, J. H. (2012). “Identification of the transmitter and receptor mechanisms responsible for REM sleep paralysis.” Journal of Neuroscience, 32(29), 9785–9795.
- Valli, K., et al. (2021). “The threat simulation theory of sleep paralysis hallucinations: Evidence from a systematic review.” Consciousness and Cognition, 95, 103209.
- Jalal, B., & Hinton, D. E. (2015). “Sleep paralysis among Egyptian college students: Association with anxiety symptoms (PTSD, trait anxiety, pathological worry).” Journal of Nervous and Mental Disease, 203(11), 871–875.
- Cheyne, J. A. (2003). “Sleep paralysis and the structure of waking-nightmare hallucinations.” Dreaming, 13(3), 163–179.
Cross-Cultural and Anthropological Sources
- Davies, O. (2003). “The nightmare experience, sleep paralysis and witchcraft accusations.” Folklore, 114(2), 181–203.
- Adler, S. R. (2011). Sleep Paralysis: Night-mares, Nocebos, and the Mind-Body Connection. Rutgers University Press.
- Hufford, D. J. (1982). The Terror That Comes in the Night: An Experience-Centered Study of Supernatural Assault Traditions. University of Pennsylvania Press.
Contemplative and Esoteric Sources
- Wangyal, T. (1998). The Tibetan Yogas of Dream and Sleep. Snow Lion Publications.
- LaBerge, S. (1985). Lucid Dreaming: The Power of Being Awake and Aware in Your Dreams. Jeremy P. Tarcher.
Safety Notice: This article explores sleep paralysis and other threshold states between waking and sleeping. It does not constitute medical, psychological, or spiritual advice. If you experience sleep paralysis frequently and it produces persistent anxiety, sleep disruption, or trauma symptoms, consult a sleep specialist or mental health professional. Sleep paralysis can coexist with narcolepsy and other sleep disorders that require clinical assessment. Contemplative frameworks complement but do not replace medical or psychological treatment. Do not attempt to induce sleep paralysis or out-of-body experiences if you have a history of psychosis, dissociation, or severe anxiety without guidance from a qualified teacher and appropriate clinical support.



