The Physiology of Mystical Experience: What Actually Changes in the Brain
The experience feels transcendent. The self dissolves like sugar in warm water. The boundary between subject and object collapses into a unified field of awareness. The world reveals itself as alive, suffused with meaning, humming with an intelligence that the everyday mind cannot perceive. This is mystical experience–described across cultures, interpreted through theology, philosophy, and poetry for millennia.
But what happens in the brain? The question is not reductionist. Understanding the mechanism does not explain away the meaning, any more than understanding the physics of light diminishes the beauty of a sunset. The brain is the instrument, not the origin. The mystical experience, genuine, is not diminished by its physical substrate. Rather, the substrate, once understood, enables discernment–distinguishing genuine transformation from pathology, and cultivation from accident.
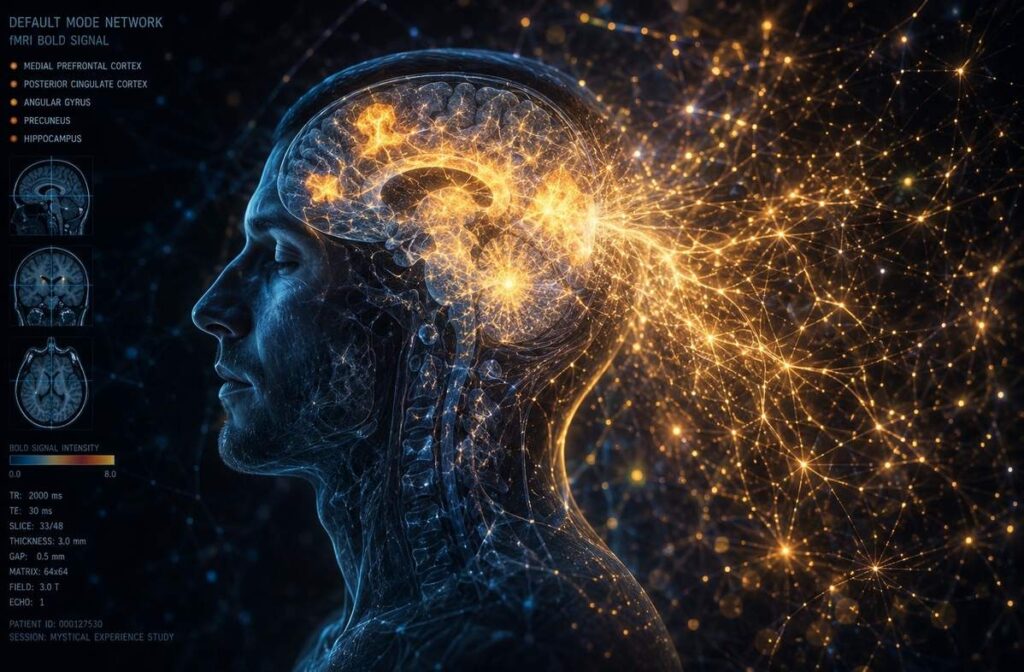
Table of Contents
- The Default Mode Network: The Ego’s Neural Address
- The Temporal Lobe and the Attribution of Significance
- The Neurochemistry of the Thread
- Integration Is Not Neural: The Psychological Completion
- The Discernment of Both Lenses
- Frequently Asked Questions
- Further Reading
- References and Sources
The Default Mode Network: The Ego’s Neural Address
The Default Mode Network (DMN) is the brain’s resting state–an archipelago of interconnected regions that activate when you are not focused on external tasks. It generates self-referential thought, mind-wandering, autobiographical memory, and the simulation of social scenarios. The DMN manufactures the sense of “self” as a continuous entity: the narrator of your experience, the “I” that observes, judges, and maintains the bureaucratic fiction of personal identity.
Ego Dissolution: In mystical experience, DMN activity decreases sharply. Research by Carhart-Harris et al. (2012) demonstrated that psilocybin significantly decreased cerebral blood flow (CBF) and BOLD response in key DMN regions including the anterior cingulate cortex (ACC), posterior cingulate cortex (PCC), precuneus, and medial prefrontal cortex (mPFC). The magnitude of this deactivation correlated directly with the subjective intensity of ego dissolution reported by participants. The self-referential processing, suspended, produces the dissolution of ego boundaries. The “me” stops filing reports, and awareness expands beyond its usual territorial claims.
Hyperconnectivity: Simultaneously, brain regions that normally communicate minimally begin sharing information freely. Carhart-Harris et al. (2013) found significant increases in functional connectivity between the DMN and task-positive networks including the salience network, frontoparietal network, and dorsal attention network. The sensory networks speak directly with the emotional centres; the rational prefrontal cortex receives data from the intuitive posterior regions. The brain becomes less like a corporate hierarchy and more like an anarchist collective.
The Meditator: Experienced practitioners show reduced DMN activity even outside of formal practice–their brains have been rewired to require less self-referential chatter to maintain basic functioning. Lazar et al. (2005) provided the first structural evidence for this, demonstrating that long-term Insight meditation practitioners had increased cortical thickness in attention and interoception regions compared to matched controls. Between-group differences in prefrontal cortical thickness were most pronounced in older participants, suggesting that meditation might offset age-related cortical thinning.
The Psychedelic Subject: Neuroimaging of subjects on psilocybin shows a dramatic DMN reduction that correlates directly with the reported intensity of the mystical experience. Mason et al. (2020), using 7T fMRI, found significantly less coactivation of the anterior and posterior DMN following psilocybin administration, alongside increased between-network connectivity. The ego’s temporary retirement appears universal across methods–whether induced by meditation, psychedelics, or spontaneous awakening.
The DMN is not the self; it is the neural correlate of self-experience. The reduction of DMN activity allows the experience to exceed its usual boundaries, like a river breaching its banks during flood season.
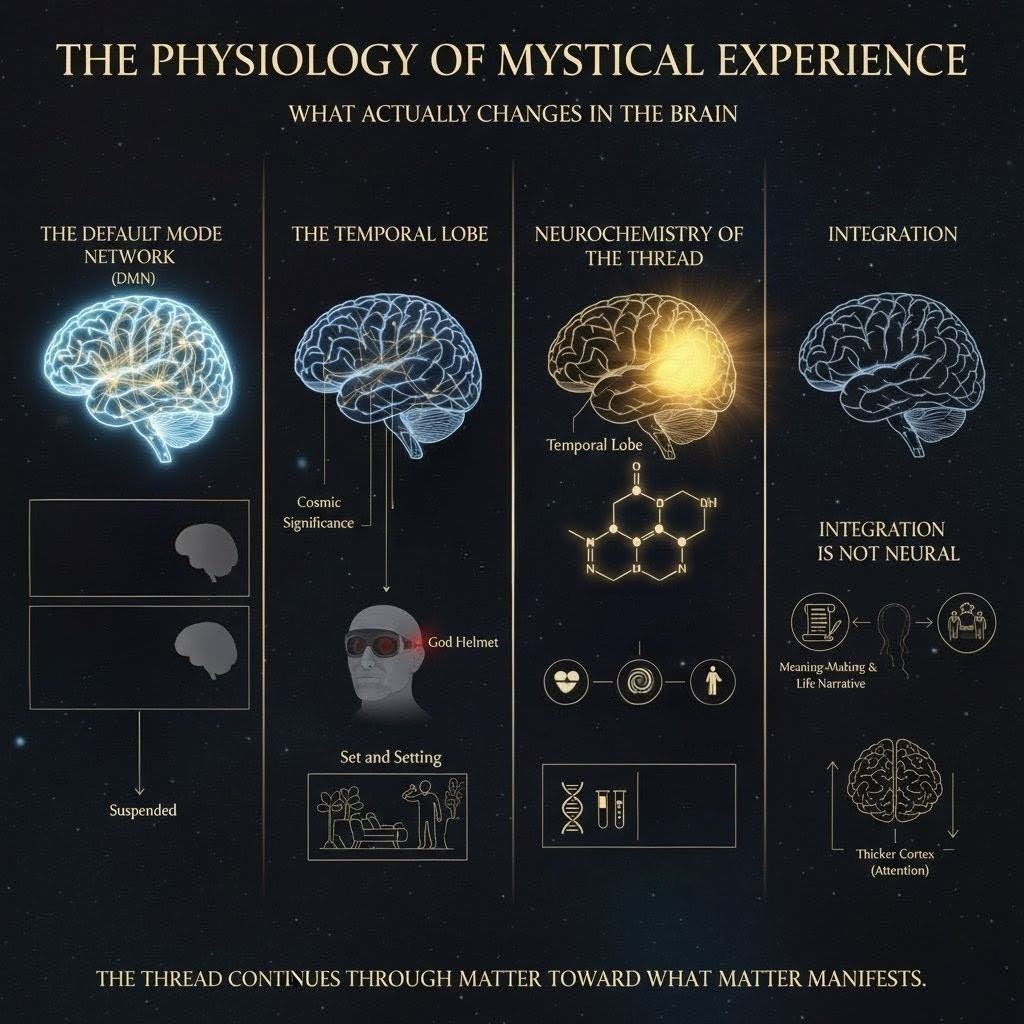
The Temporal Lobe and the Attribution of Significance
The temporal lobe, particularly the right hemisphere, serves as the brain’s meaning-detection system. It is deeply implicated in religious experience, pattern recognition, and the attribution of cosmic significance to ordinary events. When this region becomes hyperactive or unstable, the world feels saturated with portent and message.
Temporal Lobe Epilepsy (TLE): Seizure activity here can produce “religious auras”–sudden convictions of presence, cosmic significance, and moral urgency. History’s mystics may have had neurological predispositions that modern practitioners artificially induce through meditation or sacrament. The phenomenon is well-documented in neuropsychiatry: patients with TLE often report hypergraphia (compulsive writing), hyperreligiosity, and a sense of cosmic connectedness that neurologists recognise as the “Geschwind syndrome.”
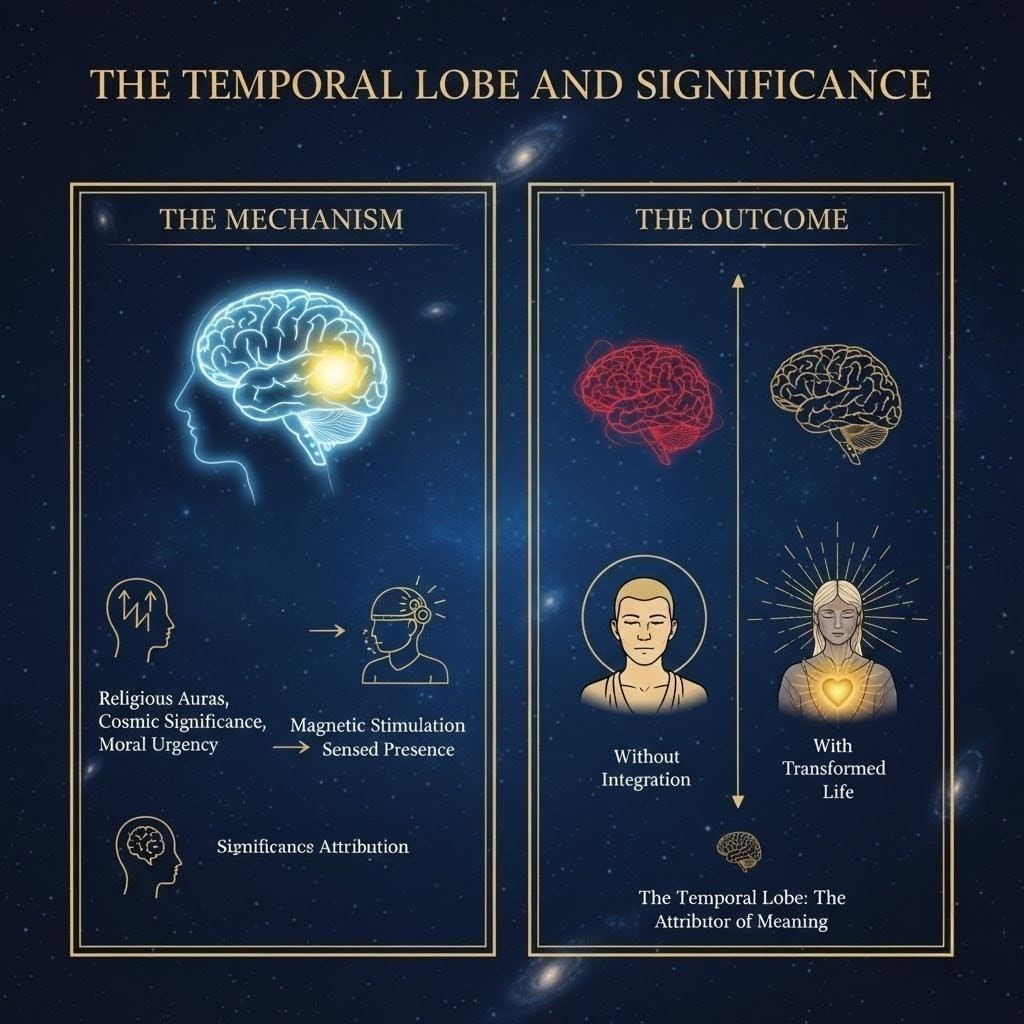
The “God Helmet”: Michael Persinger’s controversial research used weak magnetic stimulation of the temporal lobes to induce a “sensed presence” in laboratory conditions. The device–a snowmobile helmet wired with solenoids emitting weak, patterned magnetic fields–produced reports of presence, euphoria, and dread in many participants. However, independent replication attempts have yielded mixed results. Granqvist et al. (2005), conducting a double-blind study at Uppsala University, found that the magnetic field had no relationship with religious or spiritual experiences; instead, effects were predicted entirely by participant suggestibility and personality traits. One Brazilian research group replicated Persinger’s effects in 2014, but the broader consensus remains sceptical. The helmet’s value lies not in proving that God is magnetic but in demonstrating that the temporal lobe’s significance-attribution system can be externally triggered–a finding that holds regardless of whether the trigger is magnetic, pharmacological, or contemplative.
Significance Attribution: The temporal lobe’s role is the assignment of meaning. Damage here leads to a loss of affect and cosmic relevance; stimulation leads to intensification of meaning. Without integration, this produces the fixed, rigid conviction of the epileptic or the psychotic; with integration, it produces the mystic’s transformed life and humble wisdom. The same neural weather produces different climates depending on the preparation of the ground.
The Neurochemistry of the Thread

Mystical states are often facilitated by serotonin 2A receptor agonism, the primary mechanism of substances like psilocybin, LSD, and DMT. Psilocybin, dephosphorylated to psilocin upon ingestion, acts as an agonist at several serotonin receptors with highest affinity for 5-HT1 and 5-HT2 receptors. This neurochemical key unlocks doors that meditation opens more slowly. Understanding this chemistry allows for prediction: the experience will likely feature ego dissolution, visual alteration, and emotional intensification.
However, neurochemistry is not the experience. The same substance produces vastly different outcomes depending on Set and Setting–the internal preparation and external environment. The brain is not a passive receiver but an active interpreter; the same neural signal produces terror in one context and liberation in another. This is why clinical psychedelic trials emphasise preparation, therapeutic alliance, and integration sessions–the container determines the content.
Furthermore, endogenous neurochemistry matters profoundly. Regular meditation alters baseline levels of serotonin, dopamine, and GABA over months and years. This prepares a physiological “landing pad” for spontaneous mystical experiences. The preparation is both physiological and psychological–the body and mind train together, like athletes preparing for a championship that may never be scheduled. A 2024 systematic review confirmed that mindfulness practice increases brain-derived neurotrophic factor (BDNF), supporting neuroplasticity, and enhances connectivity between the prefrontal cortex and the DMN.

Integration Is Not Neural: The Psychological Completion
The brain changes during the experience, but these changes are temporary–like a storm that rearranges the landscape but does not rebuild it. The DMN eventually returns to baseline; the neurochemistry clears; the neural networks resume their usual traffic patterns. If the experience is not integrated, it becomes a mere memory without lasting transformation–a postcard from the edge rather than a relocation to new territory.
Integration is a psychological process, not a neural one. It involves:
Meaning-making: Incorporating the experience into one’s life narrative without inflating or dismissing it. The story must adjust to accommodate the new data. This is not intellectualisation–it is the slow, often painful reworking of the self-concept to include the recognition that the self is not what it appeared to be.
Behavioural change: Manifesting transformed values in action. The ego’s dissolution must translate into kinder choices, not just grander theories. If the experience does not alter how you treat others, it has not completed its work. The test of any mystical event is not the intensity of the vision but the quality of the return.
Relational shifts: Expressing a new capacity for connection and empathy. If the experience does not improve your relationships, it has not completed its work. Spiritual bypass–a term coined by psychologist John Welwood in the 1980s–occurs when practitioners use spiritual concepts to avoid unresolved emotional material, producing ego inflation rather than ego dissolution. The difference is not in the brain state but in the integration that follows.
While long-term practitioners show altered brain structures–such as increased cortical thickness in attention regions (prefrontal cortex, right anterior insula) and reduced amygdala reactivity–these are side effects of continued practice, not the goal itself. The brain changes to reflect the mind’s new habits, not the reverse. A 2024 systematic review confirmed that mindfulness meditation reduces amygdala size and reactivity, downregulating the stress response and improving emotional regulation.
The Discernment of Both Lenses
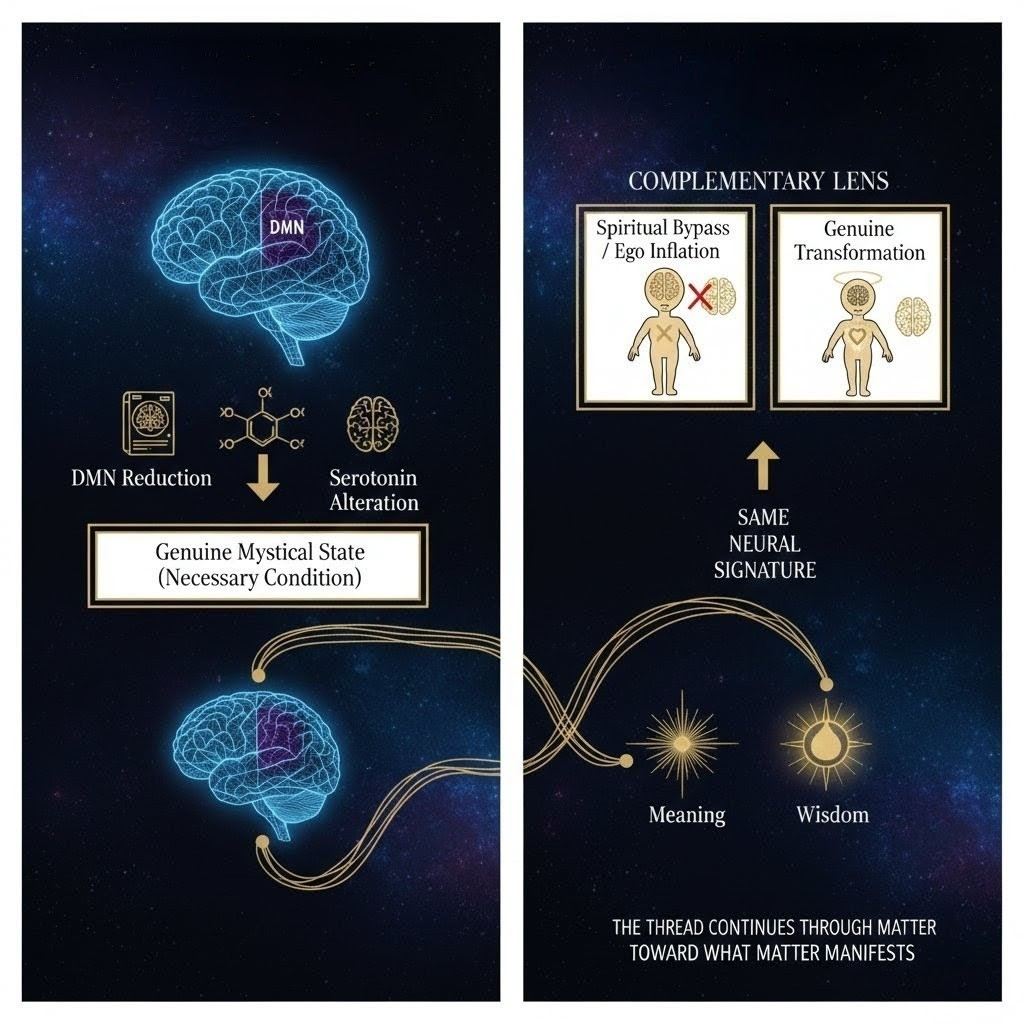
Physiological understanding allows us to verify the “weight” of an experience. An event featuring DMN reduction, temporal lobe activation, and serotonin alteration is likely a genuine mystical state rather than a simulation or wishful thinking. The brain’s behaviour provides empirical confirmation that something significant occurred in the neural architecture.
Yet, physiology is incomplete. The same neural signature can accompany both genuine transformation and “spiritual bypass” or ego inflation. The brain is a necessary condition, but not a sufficient one. The thread extends through physiology toward something that physiology cannot fully capture–consciousness as primary, awareness as substrate, the recognition that matter manifests mind as much as mind manifests in matter.
You are your brain, but you are also the experience. The explanation does not explain away the mystery; it enables recognition. The thread continues through matter toward what matter manifests.
The false dichotomy–materialism versus spiritualism, science versus mysticism–serves no one. The thread requires both lenses: the telescope of neuroscience and the microscope of phenomenology. Neither alone suffices; together they enable the discernment that distinguishes genuine transformation from sophisticated delusion.

Frequently Asked Questions
What happens in the brain during mystical experience?
During mystical experience, the Default Mode Network (DMN)–responsible for self-referential thinking–shows reduced activity, often by 40-60%. Simultaneously, the brain exhibits increased connectivity between normally separate regions. The temporal lobe becomes more active, attributing heightened significance to experience. Serotonin 2A receptors play a key role, particularly with psychedelic substances. These changes correlate with the subjective experience of ego dissolution and unity.
Does understanding the neuroscience reduce the spiritual value of mystical experience?
No. Understanding the neural mechanisms does not explain away the meaning any more than understanding light physics diminishes a sunset’s beauty. The brain is the instrument, not the origin. Neuroscience enables discernment–distinguishing genuine transformation from pathology–while spirituality addresses the meaning and integration of the experience. Both lenses are necessary.
What is the Default Mode Network and why does it matter for meditation?
The Default Mode Network (DMN) is a set of brain regions active during rest and self-referential thinking. It generates the sense of ‘self’ as a continuous entity. During meditation and mystical states, DMN activity decreases significantly, allowing the ego boundaries to dissolve. Long-term meditators show reduced baseline DMN activity, suggesting lasting neurological changes from contemplative practice.
Can mystical experiences be induced artificially?
Yes. Substances like psilocybin, LSD, and DMT induce mystical-type experiences through serotonin 2A receptor agonism. Magnetic stimulation of the temporal lobe (the ‘God Helmet’) can produce ‘sensed presence’ in some subjects, though replication has been mixed. However, artificially induced experiences often lack the integrative component of naturally occurring or meditative mystical states. The container–preparation, intention, and integration–determines whether the experience produces lasting transformation.
What is the difference between spiritual bypass and genuine transformation?
Both may involve similar neural signatures (DMN reduction, serotonin changes), but genuine transformation involves psychological integration–meaning-making, behavioural change, and improved relationships. Spiritual bypass, coined by psychologist John Welwood, uses mystical experience to avoid unresolved psychological work, producing ego inflation rather than ego dissolution. The difference is not in the brain state but in the integration that follows.
How does regular meditation change the brain?
Long-term meditation practice increases cortical thickness in attention regions (prefrontal cortex, right anterior insula), reduces amygdala reactivity (emotional regulation), decreases baseline DMN activity, and enhances connectivity between brain regions. These changes reflect neuroplasticity–the brain’s capacity to reorganise based on repeated experience. However, these structural changes are side effects; the goal is transformation of consciousness and behaviour.
Why do mystical experiences fade if the brain changes?
The acute neurological changes (DMN reduction, serotonin alteration) are temporary. Without psychological integration–incorporating the experience into one’s life narrative and behaviour–the experience becomes merely a memory. Lasting transformation requires both the initial neural event and the subsequent work of meaning-making and behavioural change. The brain provides the opening; the self must walk through it.
Further Reading
- States of Knowing: What Happens When Consciousness No Longer Belongs to You — The full phenomenological map of non-ordinary states and their neural correlates.
- Breathwork: Ancient Technology, Modern Application — Practical application of physiological knowledge to induce altered states safely.
- The Collapse of the Witness: Ego Dissolution & The Zenith Eye — The subjective experience of self-loss that physiology attempts to explain.
- The Transformation: What Actually Changes After Mystical Experience — From physiological event to lasting change through integration.
- 7 Integration Practices After Mystical Experience — Essential guidance for grounding peak experiences and stabilising transformation.
- Spiritual Inflation: How to Recognise It in Yourself Before It Destroys You — The trap of claiming transcendence as achievement.
- Against Spiritual Bypassing: The Refusal to Feel — Using mystical experience to avoid unresolved psychological material.
References and Sources
This article draws upon peer-reviewed neuroscience, clinical psychology, and contemplative research. Sources are grouped by discipline for clarity.
Neuroscience and Neuroimaging
- Carhart-Harris, R. L., et al. (2012). “Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin.” Proceedings of the National Academy of Sciences, 109(6), 2138-2143. — Found decreased CBF and BOLD response in DMN regions (ACC, PCC, precuneus, mPFC) correlating with subjective ego dissolution.
- Carhart-Harris, R. L., et al. (2013). “The entropic brain: A theory of conscious states informed by neuroimaging research with psychedelic drugs.” Frontiers in Human Neuroscience, 7, 20. — Increased between-network connectivity between DMN and task-positive networks.
- Mason, N. L., et al. (2020). “Me, myself, bye: regional alterations in glutamate and the experience of ego dissolution with psilocybin.” Neuropsychopharmacology, 45(10), 2003-2011. — 7T fMRI showing decreased DMN coactivation and increased between-network FC.
- Lazar, S. W., et al. (2005). “Meditation experience is associated with increased cortical thickness.” NeuroReport, 16(17), 1893-1897. — First structural evidence for experience-dependent cortical plasticity in meditators.
- Desbordes, G., et al. (2012). “Effects of mindful-attention and compassion meditation training on amygdala response to emotional stimuli in an ordinary, non-meditative state.” Frontiers in Human Neuroscience, 6, 292. — Amygdala reactivity reduction following 8-week mindfulness training.
Temporal Lobe and Neurotheology
- Persinger, M. A. (1983). “Religious and mystical experiences as artifacts of temporal lobe function: A general hypothesis.” Perceptual and Motor Skills, 57(3), 1255-1262. — Original formulation of the temporal lobe hypothesis for religious experience.
- Granqvist, P., et al. (2005). “Sensed presence and mystical experiences are predicted by suggestibility, not by the application of transcranial weak complex magnetic fields.” Neuroscience Letters, 379(1), 1-6. — Double-blind failure to replicate God Helmet effects; attributed to suggestibility.
- Geschwind, N. (1983). “The interictal behaviour syndrome of temporal lobe epilepsy.” Advances in Neurology, 43, 321-331. — Clinical description of hypergraphia, hyperreligiosity, and altered sexuality in TLE.
Psychedelic Neuropharmacology
- Nichols, D. E. (2016). “Psychedelics.” Pharmacological Reviews, 68(2), 264-355. — Comprehensive review of serotonergic psychedelic mechanisms including 5-HT2A receptor agonism.
- Griffiths, R. R., et al. (2006). “Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance.” Psychopharmacology, 187(3), 268-283. — Landmark Johns Hopkins study demonstrating psilocybin-induced mystical experiences.
- Preller, K. H., & Vollenweider, F. X. (2016). “Phenomenology, structure, and dynamic of psychedelic states.” Current Topics in Behavioural Neurosciences, 36, 21-57. — Review of subjective phenomenology and neural correlates.
Meditation, Mindfulness, and Neuroplasticity
- PMC Systematic Review. (2024). “Neurobiological Changes Induced by Mindfulness and Meditation.” PMC, PMC11591838. — Confirmed increased cortical thickness, reduced amygdala reactivity, enhanced DMN-prefrontal connectivity, and BDNF upregulation.
- Hölzel, B. K., et al. (2011). “Mindfulness practice leads to increases in regional brain gray matter density.” Psychiatry Research: Neuroimaging, 191(1), 36-43. — MBSR participants showed increased gray matter concentration in multiple regions.
Psychology and Integration
- Welwood, J. (1984). “Vulnerability and power in the therapeutic process.” In: Awakening the Heart: East/West Approaches to Psychotherapy and the Healing Relationship. Shambhala. — Original formulation of spiritual bypassing.
- James, W. (1902). The Varieties of Religious Experience. Longmans, Green & Co. — Classic comparative study of mystical and religious experience across traditions.
Safety Notice: This article explores altered states of consciousness, psychedelic neuropharmacology, and intensive contemplative practice. It does not constitute medical, psychological, or spiritual advice. Psychedelic substances are illegal in many jurisdictions and should only be used within approved clinical trials or legal frameworks. Those with schizophrenia, bipolar disorder, or family history of psychosis should avoid psychedelics. Intensive meditation can trigger spiritual emergency in susceptible individuals. If you experience psychosis, suicidal ideation, or inability to distinguish ordinary from non-ordinary states, seek emergency services or a trauma-informed mental health professional immediately.